ACUTE LARYNGOTRACHEOBRONCHITIS(CROUP) D K JHA,MD
Acute laryngotracheobronchitis (croup)
:INTRODUCTION
> It is the most common cause of acute upper airway obstruction in children.
> Usually affects children between 3 months to 3 years of age.
> Most common affected age group is 18 months to 24 months.
> Usually occurs during winter and falls but may occur during any season of the year.
> Most common causative agent is parainfluenza virus 1(PAV1),responsible for epidemics.
> Other agents are PAV2,PAV3,RSV,RV,Human metapneumovirus,maesles virus, and mycoplasma.
CASE SUMMARY:
Nand Lal is a 2 years and 8months old male child presented in our emergency department with loss of consciousness 60 minutes back when he was playing outside of his house near the door.The loss of consciousness was for a brief period of few seconds when his father noticed while he was going out for market.When the father picked him up ,the child regained consciuosness but not fully and his breathing pattern was different from normal and was noisy.When I examined the child in the emergency,his SPO2 on room air was 82% ,breathing pattern was irregular with a rate of 90/minute,heart rate was 144/minute,regular.Chest on auscultation revealed biphasic stridor. The child was a known case of congenital micrognathia.I diagnosed the child as a case of CROUP,although foreign body aspiration was a strong possibility. Child was admitted in ICU.The child responded well to treatment and discharged after 72 hours.
: CLINICAL FEATURES
> Common presentation is running nose ,sneezing ,cough which worsens over 2-3 days and becomes barking.
> cry or voice becomes hoarse over 2-3 days or parents may notice some change in quality of voice or cry.
> Fever is usually mild for 2-3 days but fever in the range of 102-104 degree F may be observed.
> Symptoms tend to worsen during evening and night.
> There may be signs and symptoms of URI in family members.
> Stridor is the hallmark clinical sign of croup which is recognized as harsh vibratory sound of variable pitch caused by partial obstruction of respiratory passage that result in turbulent airflow through airway.
> Stridor can be inspiratory ,expiratory or biphasic meaning both in inspiration and expiration depending upon the site and type of airway obstruction.
> In croup, stridor is inspiratory ,which is harsh ,high pitched sound produced when child inspire through a spasmodically closed glottis.
> There is Westley clinical croup score to categorise it into mild ,moderate and severe croup but broadly it can be categorized as
> MILD : if the child is active ,interactive ,alert and taking feed normally and no stridor at rest but stridor appears once the child crys or exerts and there is no sign of respiratory distress.
>MODERATE :if the child is alert ,active ,interactive but can take only liquids orally,stridor present at rest as well as a degree of respiratory distress in the form of chest wall recession and tachypnea.There is usually accompanying tachycardia.
>SEVERE:Progression from moderate to severe can become rapidly and may be precipitated by distress caused by clinical examination.Worrysome signs include increasing respiratory distress,anxious and tired look but not toxic look,drooling may occur and child refuse even liquids or may be unable to coordinate swallowing and breathing,there may be agitation ,restlessness,pallor ,cyanosis and decreased level of consciousness but spo2 may well be preserved till late stage of airway obstruction in absence of lower airway involvement.
DIAGNOSIS:The diagnosis is chiefly clinical.
throat examination may show pharyngeal inflammation
Laryngoscopic examination should be avoided as the patient may deteriorate suddenly and may need intubation to save life.
X-RAY-Neck Xray antero-posterior view may show steeple sign of airway narrowing or may be completely normal.Moreover,this steeple sign may be seen in some normal children.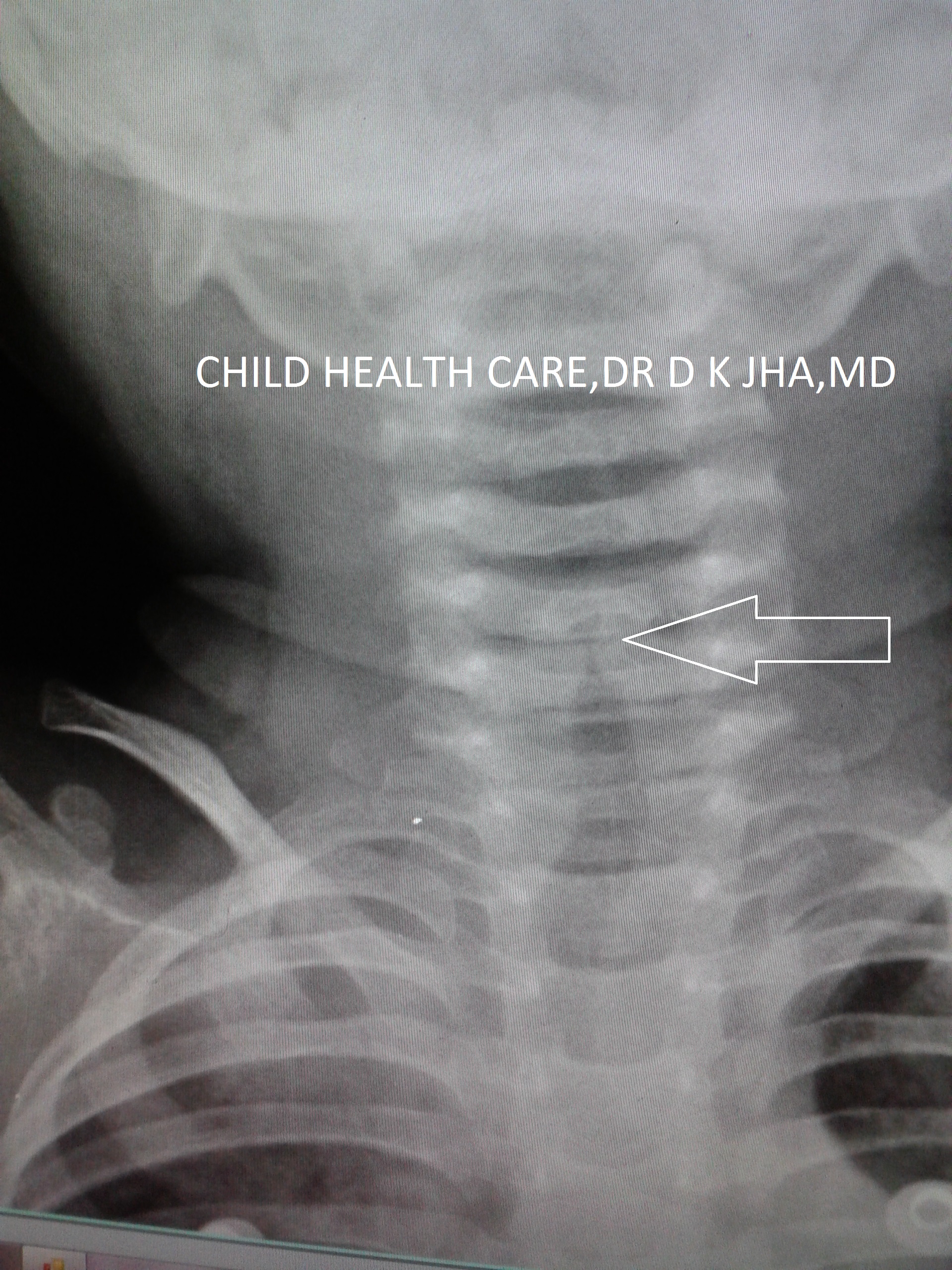
Isolation of virus in laboratory is not useful as it does not change the mode of treatment.It is useful only for research purpose.
:TREATMENT
> Mild cases can be managed at home with symptomatic treatment and oral prednisolone in the dose of 1mg/kg body wt per day for 2 days,Paracetamol for fever ,saline nasal drop for nasal clearance in infants with no cough formulations and no antibiotics.
>Moderate cases should be given dexamethasone im or iv in the dose of 0.3 to 0.6 mg /kg body wt and observed at interval of 30 minutes ,if improved to mild category at 6hours send home with symptomatic treatment as this steroid dose will act for 2-3 days.
OR
Nebulize with Adrenaline(l adenaline) 0.5ml/kg body wt upto a maximum of 2.5 ml for children less than 4 years and 5 ml for more than 4years of age.Racemic adrenaline(mixture 1:1 of l adenaline and d adrenaline) is available at selected centres of world but L-Adrenaline which is widely available is equally good.Its action starts within 30 minutes and lasts for 2-3 hours
>Hospitalize children if more than one nebulization is required.Nebulization can be done with adrenaline alone 1:1000 solution but normal saline should be mixed to make the nebulizing solution at least 3ml if the total dose is less than it.
>If child fails to respond as expected, consider other diagnosis like retropharyngeal abscess.bacterial tracheitis,epiglottitis,sub glottis stenosis or foreign body.
ALTERNATIVE TREATMENT:
Nebulizatin with 2 mg budesonide ,upto 4 doses 12 hourly depending on response.
: INDICATIONS FOR HOSPITALIZATION
> Progressive stridor,severe stridor at rest, respiratory distress,hypoxia,depressed mental status, cyanosis,poor oral intake and need for reliable observation.
TREATMENT IN HOSPITAL
> Hospitazized children should be treated with iv fluid,oxygen even if not hypoxic and in respiratory distress, to give rest to respiratory muscles,
> dexamethasone can be repeated 6 hourly upto 4 doses according to need.
> adrenaline nebulization can be repeated 2-4 hourly according to need
> antibiotics should be considered only if there is evidence of secondary bacterial infections.
REFERENCES:
-
: Inhalation of racemic adrenaline in the treatment of mild and moderately severe croup: clinical symptom score and oxygen saturation measurements for evaluation of treatment effects.Acta Pediatr. 83:1156–1160 1994
-
: Outpatient treatment of moderate croup with dexamethasone: intramuscular versus oral dosing. Pediatrics. 106:1344–1348 2000 11099587
-
: Controlled delivery of high vs low humidity vs mist therapy for croup in emergency departments. JAMA.295:1274–1280 2006 16537737
-
: Prospective randomized double-blind study comparing l -epinephrine and racemic epinephrine aerosols in the treatment of laryngotracheitis. Pediatrics. 89:302–306 1992 1734400
-
: Utility of radiographs in the evaluation of pediatric upper airway obstruction. Ann Otol Rhinol Laryngol. 108:378–383 1999 10214786
Tags: ADRENALINE, CROUP, STRIDOR